
C.A.B.S. Birth Blog |
|
In the local breastfeeding support groups one of the most common questions is “Is drug X compatible with breastfeeding?” It can be really confusing! The medical field is full of contradicting advice when medications and breastfeeding are involved. There is always worry about potential harm to baby from medications going into breast milk that many care providers take a “no drug is safe while breastfeeding” approach, while others say to “pump and dump” for days following a procedure. This doesn't help breastfeeding parents figure out what's best, and has the potential to damage a breastfeeding relationship for no reason if an uneducated opinion is given. **Hint: if someone tells you you should not breastfeed while taking a certain medication, ask them how much education they have on breastfeeding! This post is not meant to be a database of drugs and breastfeeding compatibility (any decisions on medication and breastfeeding should be carefully discussed with your lactation consultant AND medical provider). Your provider may not know everything about how the drug interacts with milk and breastfeeding. Your Lactation Consultant probably will. That's why it is important to have both of them in the conversation. There are new drugs being introduced frequently and many of them have not been tested for compatibility with breastfeeding. This is to help you understand the basics of how your body makes milk, how drugs enter human milk in varying amounts, and how you can find out more information about drugs so you can discuss them with some level of confidence. To understand why certain medications are safe to take while breastfeeding while others are not requires knowledge of the process of how the human body makes milk and how different medications are processed by the body.  There are several ways that drugs can find their way into breast milk. What are the main ways drugs do this? The following list describes the most common methods drug transfer from the breast into the milk. Note that not all drugs are processed in these ways and some drugs get into milk using more than one of these methods. It is also worth of noting that during the first few weeks of lactation the tissue of the breast is very porous and there is a greater amount of space between the cells that produce the milk which makes it easier for more drugs to pass through. What determines how much of a drug baby is exposed to:How the drug enters your body:We put drugs on our skin, in our mouths, we inhale them, and even get them through IVs. The way a drug enters the body can be important. Most drugs that are applied to the skin (topically) do not enter the bloodstream easily thus do not find their way into milk in any amount that would be a cause for concern. Many inhaled drugs are the same and do not absorb easily. Oral and intravenous (through an IV) applications tend to get more significant drug amounts into the blood and milk but not always. The makeup of the drug and the way it is processed all have to do with how it gets into milk and if it stays there for long periods. plasma level:This is the most important factor in determining the potential of a drug transferring into milk. The higher the maternal plasma level of the drug, the more likely it is that some of the medication has made its way into the milk due to a process called passive diffusion. It can be a bit confusing so I will try to keep it simple. Here's a bit how that works: To make milk the breasts must get fluid from the body. This fluid is taken from the blood-particularly the plasma, but if the plasma wants to make it into the milk compartment it needs to go through the tissue. Milk glands have what's called a semi permeable membrane. That basically means the milk gland works as a bouncer at a club, only molecules of certain shapes and sizes are allowed in. Think of the bloodstream as the admission line and the milk compartment of the milk gland as the club. 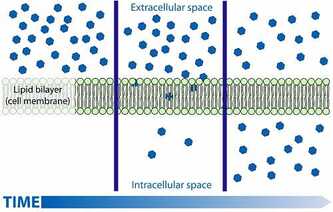 https://biologydictionary.net/passive-transport/ https://biologydictionary.net/passive-transport/ When the breastfeeding person's plasma meets the newly forming milk, the stuff that's in the plasma, including the drug, want to move from an area where it is highly concentrated (the bloodstream) to an area where it is of lower concentration (the milk compartment) because of passive diffusion. Basically the bouncer may fall for that drug's fake ID and let it in if it looks legit. So if the structure of the drug makes it too big to fit, it can't get into the milk. If some of the drug is able to it will cross the membrane and find its way into the milk it will, but milk concentrations will almost never become higher than the maternal plasma level either due to passive diffusion. If a breastfeeding person has a high plasma level of the drug, it is likely that the drug is present in the breast milk in significant amounts for some amount of time until the concentration peaks and is then being processed out of the body, and then the drug will begin to cross the membrane again, this time leaving the milk as the body processes it out. Lipid solubility:Lipid is a scientific word for fats. If a drug clings to fat easily, the easier it is for it to pass through the cell and store in the milk. Lipid soluble drugs can also store in the breastfeeding person's body fat and be released into the bloodstream if they burn fat. Bioavailability:Bioavailability is the ability for a drug to survive the digestive system and make it into the circulatory system (blood stream). Many drugs are simply not able to survive the harsh environment and make it into the blood or milk in significant levels. Molecular Weight of the medication:The more weight to the drug, the more difficult it is for it to travel through the lactocytes (milk producing cells) and into milk. Half-life: The half-life of a given medication is how long it takes for the body to get rid of half of the dose. After the medicine concentration in the blood peaks it begins to process out of the body. This length of time varies and can have a big impact on how long a medication stays in the milk. Amount of milk and amount of drug:The safety of a drug while breastfeeding also has to do with the amount of milk your baby drinks. If baby is exclusively breastfeeding they will get more of the drug but if a baby is older and eating solids with only a few nursing sessions/day then they will receive significantly less of the drug. Some people consider milk a “living” liquid since it is full of active beneficial bacteria, immune properties, and breastfeeding person's cells. Since milk welcomes so many beneficial things for baby from the breastfeeding person's body into it there is room for other substances like drugs to sneak in. If a nursing person needs to take a medication research into the safety of the drug should be done by that person, their lactation consultant, and physician to determine if the drug would be safe for them and baby. Ultimately the choice is up to the breastfeeding person to either withhold from the drug, to pump and remove discard the milk when the concentration in the milk is at a peak, or continue breastfeeding as normal. This choice should be an informed and educated one, not one made through generalization and guesses. My hope is that this article breaks down the basics of drugs and breastfeeding and gives you a better understanding of the many different factors to consider when introducing a drug into your breastfeeding relationship. For more information on safety of medications you can visit the Drugs and Lactation online database by clicking the button below: Bibliography
Riordan, J. (2005). Breastfeeding and Human Lactation. Jones and Bartlett .
0 Comments
|
AuthorHi, Jessie here. I'm a doula, mother, and wearer of many hats. All things birth related are my passion. It brings me great joy and satisfaction to serve clients and educate families. I am new to blogging, and excited to share with you all lots of different things about birth. Archives
May 2020
Categories |
 RSS Feed
RSS Feed
